What makes a medical translator? A survey on medical translators’ profiles, work-related challenges and use of Computer-Assisted Translation and Automatic Speech Recognition tools
Raluca Chereji1, University of Vienna
The Journal of Specialised Translation 42 (2024), 39-62
https://doi.org/10.26034/cm.jostrans.2024.5979

ABSTRACT
Advancements in healthcare and the rise of patient-centredness have increased workloads for professional medical translators. In parallel, new and emerging technologies are impacting translators’ output and workflows, though investigations into the medical translation domain remain scarce. This article presents the results of an international survey on 165 professional medical translators to identify trends concerning their socio-demographic and professional profiles, the textual- and process-related challenges of translating medical texts aimed at patients as laypersons, and their use of technology, specifically Computer-Assisted Translation (CAT) tools and Automatic Speech Recognition (ASR). Results show that the medical translators surveyed have decades-long experience in translation and come primarily from a linguistic background. They find specialised terminology and delivery deadlines as most challenging when translating patient-facing medical texts. Finally, most medical translators in our survey use CAT tools when translating or post-editing, although a small minority also integrate ASR tools into their workflows.KEYWORDS
Medical translation, translators’ profiles, medical translation challenges, Computer-Assisted Translation tools, Automatic Speech Recognition.1. Introduction
In recent years, medical translation has become an increasingly important specialism among professional translators. Industry reports rank healthcare and the related field of life sciences as the second most common translation specialism, after the legal domain (ELIA et al., 2023, p. 27; Hickey 2023). This trend is supported by the rise in academic and professional training programs in medical translation (Muñoz-Miquel, 2018, p. 25), highlighting both the market demand for professional translators and the specialisation levels required to operate in this field.
Developments in healthcare play a significant role in driving the demand for medical translation services. Within clinical research, factors including the COVID-19 pandemic and therapeutic advancements such as personalised medicine have increased the pace and number of international clinical trials. These trials generate enormous amounts of documents, from protocols and legal agreements to participant recruitment materials, and are subject to stringent regulatory requirements and time-sensitive procedures given the legal, ethical and economic risks they entail. However, while translation is necessary for most clinical trial development stages, and particularly regulatory submissions, it is “rarely given the attention that it requires” within trial planning (Maeda-Nye, 2009, as cited in Bolaños-Medina, 2012, p. 18), despite the significant consequences faulty translations may have.
Medical translators can be instrumental in the success of a clinical trial and in subsequent marketing submissions by ensuring that strict quality and regulatory requirements are met. Achieving this entails both specialised medical knowledge, particularly for technical documents aimed at medical experts (e.g., trial protocols), and intralingual adaptation skills when working on medical texts for patients and other laypersons, such as patient information leaflets (PILs) and informed consent forms (ICFs). Reflecting the rise of patient-centredness in healthcare, these documents often originate from texts written for medical experts, but target laypersons who have different comprehension needs and expectations regarding medical communication. Medical translators need to be aware of such demands and discourse shifts if they are to produce translations that are not only lay-friendly, but also comply with legal and regulatory guidelines, as failure to do so can impact patient safety. This, in turn, raises questions about the medical translators themselves and the competencies required for the field: what are their backgrounds and experience levels, their areas of expertise and the challenges they encounter when working on medical texts for patients?
The nature of the translation profession itself is also changing. Reflecting the ‘technological turn’ in translation (O’Brien & Conlan, 2018), the emergence and adoption of different tools and technologies into translators’ workflows has led to the ‘technologisation’ of translation as both profession and practice. This trend is visible in the variety of tools available on the market and in the types of tasks and use-cases for which they are being implemented across different specialisms (ELIA et al., 2023, p. 36), including medical translation. As a result, technologies such as Machine Translation (MT) and Computer-Assisted Translation (CAT) have shifted from an optional, but nice-to-have addition to a necessity (Moorkens, 2017, p. 464), if translators are to remain competitive. This, in turn, has raised productivity expectations, and applied downward pressure on costs and delivery times (Moorkens, 2017, p. 466; O’Brien & Conlan, 2018, p. 82).
While medical translation has historically evolved “hand in hand” with technological developments (Zethsen & Montalt, 2022, p. 364), research into technology usage among medical translators remains limited and focuses primarily on MT (especially training and deployment) over CAT tools. Some studies have documented medical translators’ experience of and attitudes towards using translation technologies (Gamal, 2020; Muñoz-Miquel et al., 2020; Vidrequin, 2022), but many of these focus on specific language pairs, rather than charting trends across the wider community of medical translators. Such investigations are, however, necessary to determine the current technology-assisted working practices of medical translators, given the textual- and process-related challenges they encounter.
This article aims to address these questions by presenting findings from an international survey of 165 professional medical translators. Our objectives are threefold: firstly, we assess the socio-demographic and professional features of practicing medical translators worldwide and contribute systematic data “about who translates medical texts or what features characterise their professional practice” (Muñoz-Miquel, 2018, p. 26). Secondly, we investigate the challenges inherent in translating medical texts for patients such as ICFs and PILs. Thirdly, we consider how medical translators use technology in their practice by discussing the integration of CAT tools and Automatic Speech Recognition (ASR) into their translation and post-editing workflows.
2. Background
2.1 Who translates? Understanding medical translators’ profiles
Research into translation as both a practice and a profession has long been linked to questions about the backgrounds, training, and demographic profiles of those who engage in it, whether informally or professionally. Several large-scale, language independent international surveys have charted the makeup of the community of language professionals regarding their gender distribution, years of experience, qualifications, areas of expertise, technology usage and job satisfaction (CIOL & ITI, 2011; Stokes, 2022; ELIA et al., 2023). Academic research has also provided useful insights regarding translators’ working conditions, perceptions of status, and attitudes to the profession, both internationally (Katan, 2009; Pym et al., 2012) and in local contexts (Ruokonen & Mäkisalo, 2018).
However, domain-specific evaluations of translators’ profiles are scarcer. While surveys on the global translation profession outline the proportion of translators who specialise in medicine (Katan, 2009; ELIA et al., 2023), they do not provide information about who these translators are or what backgrounds they have. Instead, research tends to address specific linguistic contexts, with considerable work into professional medical translation centred on Danish- and Spanish‑speaking linguists. Here studies have investigated the socio-professional differences between groups of medical translators, for instance, trained translators and healthcare professionals (Nisbeth Jensen & Zethsen, 2012; Nisbeth Brøgger, 2017; Muñoz-Miquel, 2018). Other research has considered the socio-economic makeup and employment situation of English-Spanish medical translators and the tasks they routinely perform (Muñoz-Miquel et al., 2020), while in the French context the focus has primarily been on medical translators’ use of technology (Martínez, 2019; Vidrequin, 2022).
These studies are important baselines for understanding the personal and professional backgrounds of practicing medical translators. However, broadening investigations beyond singular linguistic contexts is necessary to uncover trends within the wider medical translator community; this aim informs the global focus of our study.
2.2 Medical translation: issues and challenges
While translation has historically played an important role in communicating medical knowledge, recent advancements in healthcare and the emergence of specialised sub-fields such as clinical research and regulatory affairs have generated unprecedented demand for translation, and with it, considerable career opportunities for medical translators (Montalt et al., 2018; Muñoz-Miquel, 2018, p. 25).
Within academia, researchers have investigated the challenges medical translation poses to linguists in terms of both product and process. Particular attention has been paid to the nature of medical language itself, including the presence of specialised terminology, Latin-based terms, abbreviations, collocations, sentence length and syntax, and translation strategies such as explicitation or omission, depending on domain or language pairs (Simonsen, 2014; Jiménez-Crespo & Tercedor Sánchez, 2017; Buysschaert, 2021; Zethsen & Montalt, 2022). The extent to which translators find these challenges difficult has been linked to whether they are trained linguists or subject-matter experts. In a survey by Muñoz-Miquel (2018), translators with linguistic backgrounds tended to struggle more with conceptual and terminological aspects (e.g., understanding specialised concepts or using phraseology specific to their target readers), whereas translators with scientific backgrounds encountered difficulties in translating “the asymmetries that derive from differences between the healthcare cultures” (ibid., p. 41).
These issues are compounded when translating medical texts for “the general population and patients, i.e. lay people” (Nisbeth Brøgger & Zethsen, 2021, p. 97). To meet the needs and expectations of a non-expert audience, medical information needs to be adapted from the expert-to-expert communicative scenario, to an expert-to-lay context by way of intergeneric (i.e., from one text genre into another) and intralingual (i.e., within the same language) transfer (Montalt-Resurrecció & Shuttleworth, 2012; Montalt et al., 2018; Nisbeth Brøgger & Zethsen, 2021). In translation, this also requires interlingual adaptation from one language into another.
These cumulative transfers pose considerable problems to medical translators because of the inherent tension between the expert and lay contexts, and studies have documented a host of challenges in patient-facing texts such as Patient Information Sheets (PIS), PILs and ICFs. These include specialised medical jargon, passive forms and nominalisations, complex, ambiguous or lengthy syntax, and coherence and consistency issues (Zethsen & Askehave, 2010; Pilegaard & Ravn, 2013; Nisbeth Jensen & Zethsen, 2012; Sand et al., 2012; Nisbeth Brøgger & Zethsen, 2021; Zethsen & Montalt, 2022). Also important are process-related challenges. Given the legal and ethical risks associated with patient-facing communication, these text types are subject to stringent regulatory oversight from bodies including the European Medicines Agency, which requires compliance with approved template wording and layout, as well as periodic revisions and updates (Nisbeth Brøgger & Zethsen, 2021, p. 101; Karwacka, 2021, p. 88). These requirements, alongside other translation-related hurdles such as tight deadlines and incomplete project instructions, put significant pressure on medical translators who are already grappling with the challenges of a complex text type.
2.3 Established and emerging technologies in medical translation
The use of CAT and MT technologies by professional translators has been widely documented in both industry and academia (Cadwell et al., 2018; Verplaetse & Lambrechts, 2019; ELIA et al., 2023; Farrell, 2023). However, there are fewer accounts of medical translators’ experiences of and attitudes toward using translation technology. One survey on MT acceptance among French-speaking professional medical translators finds that half of the respondents refuse to use MT or perform post-editing, though overall CAT tool usage remains high (Vidrequin, 2022, p. 255). Another survey on English-Spanish medical translators finds similar MT usage trends (Muñoz-Miquel et al., 2020), with 44% of the 39 respondents taking on post-editing tasks; of these, 24% post-edit “very frequently” (ibid., p. 147). These figures, though language-specific, appear higher than those in the ELIA survey, which puts actual MT usage among professional translators at 28% (ELIA et al., 2023, p. 10). This begs the question of whether technology use among medical translators is consistent with trends observed within the translation industry.
Beyond MT and CAT tools, speech technologies have also attracted the attention of the industry and academia for their potential to shape translators’ output and work processes. Automatic Speech Recognition (ASR; also Speech-to-Text, S2T) and speech synthesis (also Text-to-Speech, T2S) allow users to produce, review and manipulate text translations using sound rather than — or in combination with — typing, which has the potential to change how established translation workflows are performed. Both types of technology have been investigated in various use-cases, with ASR used primarily to dictate translations from scratch. Studies indicate that this way of working can improve translators’ productivity (Zapata et al., 2017; Liyanapathirana & Bouillon, 2022), ergonomics (Ehrensberger-Dow & O’Brien, 2015) and accessibility for disabled and non-disabled translators alike (Ciobanu & Secară, 2019).
Within this context, there is emerging research indicating that speech recognition tools may have a positive impact on the fluency of translations in particular situations. One study by Ciobanu (2016) suggested that dictating translations using ASR can improve the fluency and naturalness of the output, particularly for longer sentences and in domains familiar to the translator. However, it may also lead to translators making more informal and colloquial translation choices than they would by typing (ibid., p. 135). Both effects may constitute an advantage when translating medical texts for patients and other laypersons: dictating ICF or PIL translations may help medical translators adhere better to lay-friendly principles, thereby improving the comprehensibility of the resulting translations. While there is a small, but growing uptake of ASR among professional translators (ELIA et al., 2023, p. 37), there is little work on whether — and how — medical translators currently use ASR in their work, despite the existence of dedicated ASR tools for the medical domain (e.g., Dragon Medical One).2
We note here that perhaps the most innovative technology to enter the translation industry is generative AI (GenAI). The impact of GenAI on medical translation and the wider translation industry is multifaceted and deserves its own discussion, especially since the release of OpenAI’s GPT-4 in March 2023 (Krüger, 2023), which occurred after the launch of our survey. Given these limitations, GenAI will not be discussed within our study.
3. Methodology
3.1 Research questions
This survey aims to identify trends within the international community of medical translators based on three research questions:
RQ1: What are the socio-demographic and professional profiles of professional medical translators?
RQ2: What are the challenges of translating patient-facing medical texts as perceived by the translators?
RQ3: How do medical translators use Computer-Assisted Translation and Automatic Speech Recognition tools in their workflows?
3.2 Study design
The design of this survey was informed by research from Muñoz-Miquel (2018) on the differences between English-Spanish medical translators with linguistic backgrounds and those with scientific backgrounds. To facilitate analysis, Muñoz-Miquel describes two types of responder information: (1) socio‑demographic data, which covers gender, age, employment status, graduate and postgraduate training, and (2) socio-professional aspects, relating to their translation activity and perceived training needs (ibid., p. 7). Since we aim for an overall understanding of our respondents’ backgrounds, we borrow these two concepts but investigate them jointly in our study under the term ‘socio-demographic and professional profile’, which includes respondents’ personal and professional information.
The target population for our survey were professional medical translators working in any language combination and/or direction and who have experience with patient-facing (i.e., aimed at patients as laypersons) medical texts. There were no restrictions regarding translators’ geographic location.
The data collection instrument was an online questionnaire designed and offered in English; the potential impact of this language choice on participation is discussed in Section 6. It consisted of 32 questions, which were ordered thematically into three sections:
Respondents’ socio-demographic and professional profiles (Q1–Q11);
Medical translation work and challenges of translating patient-facing medical texts (Q12–Q21);
Experience using CAT tools and speech technologies (Q22–Q31).
The questionnaire landing page outlined the aims of the research and its inclusion in the author’s doctoral project, contact details for the author, and the survey privacy policy, as required by the University of Vienna Ethics Committee which approved the doctoral research. It also included a final section (Q32) reiterating data protection provisions, with a comment box for any questions or data access requests from the participants, if needed.
A mix of question- and answer formats were used, given the thematic variety of the questionnaire (Gaspari et al., 2015, p. 337). These include single-choice questions (e.g., “Please indicate your age group”), multiple-choice question (e.g., “What is your current role in the translation industry?”), rankings (e.g., “What are the most challenging textual characteristics of patient-facing documents such as Informed Consent Forms and Patient Information Leaflets?”) and sliding scales (e.g., “How many years of professional medical translation experience do you have?”). The answer options provided to respondents, particularly those concerning their medical translation activity and related challenges, were developed based on the tasks and translation requirements reported as problematic in research on medical translation (e.g., Zethsen & Askehave, 2010; Pilegaard & Ravn, 2013; Ezpeleta Piorno, 2021).
Open-ended questions served to record socio‑demographic data such as countries of residence, language pairs, and areas of expertise, and allow respondents to elaborate on specific points (e.g., motivations for using ASR) or provide answers not included in the multiple-choice options. All but seven questions were compulsory, as they depended on specific answers to prior questions. Instructions and help messages were provided throughout the questionnaire.
The draft questionnaire was evaluated in-house by five experts and subsequently pilot tested by two professional medical translators whose profiles matched those of the target population of the questionnaire (Muñoz-Miquel, 2018, p. 28). Both groups provided feedback on wording, question and answer types, logical progression, questionnaire structure and length. Their suggested improvements were incorporated into the final version of the questionnaire.
The survey was open between February–June 2023 and hosted using LimeSurvey,3 a web‑based, open-source survey creation tool. It was distributed online using a snowball sampling technique (Saldanha & O’Brien, 2013, p. 34) to international translator associations, networks and platforms dedicated specifically to medical translators, translator mailing lists, professional organisations, social media channels, and shared with senior academics in medical and specialised translation, and freelance medical translators. The author sought to include non-Western perspectives and contacted translator associations in Latin America, Africa, Asia and the Middle East; translator groups in South Africa, Senegal, Ecuador and Guatemala, among others, agreed to distribute the survey.
The analysis of the results was performed using descriptive statistics such as mean, median and standard deviation (SD).
4. Results
A total of 279 responses were received, of which 166 were completed in full. One respondent did not have any translation experience, whether medical or otherwise, and was excluded from the analysis to avoid distorting the results. The 113 partial responses included 106 blank entries, one respondent who did not meet the eligibility criteria, and six respondents who completed the questionnaire in full but failed to submit their answers. All partial responses were excluded from the analysis. The below results and discussion concern the final sample of 165 medical translators.
The questionnaire completion rate was 59%. As with other questionnaires with similar approaches to dissemination (Gaspari et al., 2015, p. 338), it was not possible to calculate the response rate: while it may have been feasible to estimate membership numbers of those organisations contacted, it is impossible to know the number of those privy to newsletters, mailing lists and social media posts (ibid.).
4.1 Respondents’ socio-demographic and professional profiles
Of the total respondents, 85% were female and 13% were male, with the remaining 2% either non-binary/diverse or undisclosed. Most respondents (69%) were aged between 31 and 60 years; Table 1 lists the full breakdown of respondent age groups, with the numbers in the percentage column rounded up.
| Age group | N | % |
|---|---|---|
| 18-24 | 2 | 1% |
| 25-30 | 16 | 10% |
| 31-40 | 34 | 21% |
| 41-50 | 44 | 27% |
| 51-60 | 36 | 22% |
| 61 and over | 33 | 20% |
| Total | 165 | 100% |
Table 1. Respondents by age group.
The mean number of years of professional translation experience for the sample was 19 (SD 10.69; median 18). The least experienced respondent had one year of experience, compared to 50 for the most experienced respondent. Respondents’ experience in years, collected using a slider question, is reported in Figure 1 in 10-year increments, a threshold commonly used to discuss domain expertise (Muñoz Martín, 2014, p. 5, cited in Muñoz-Miquel, 2018, p. 34).
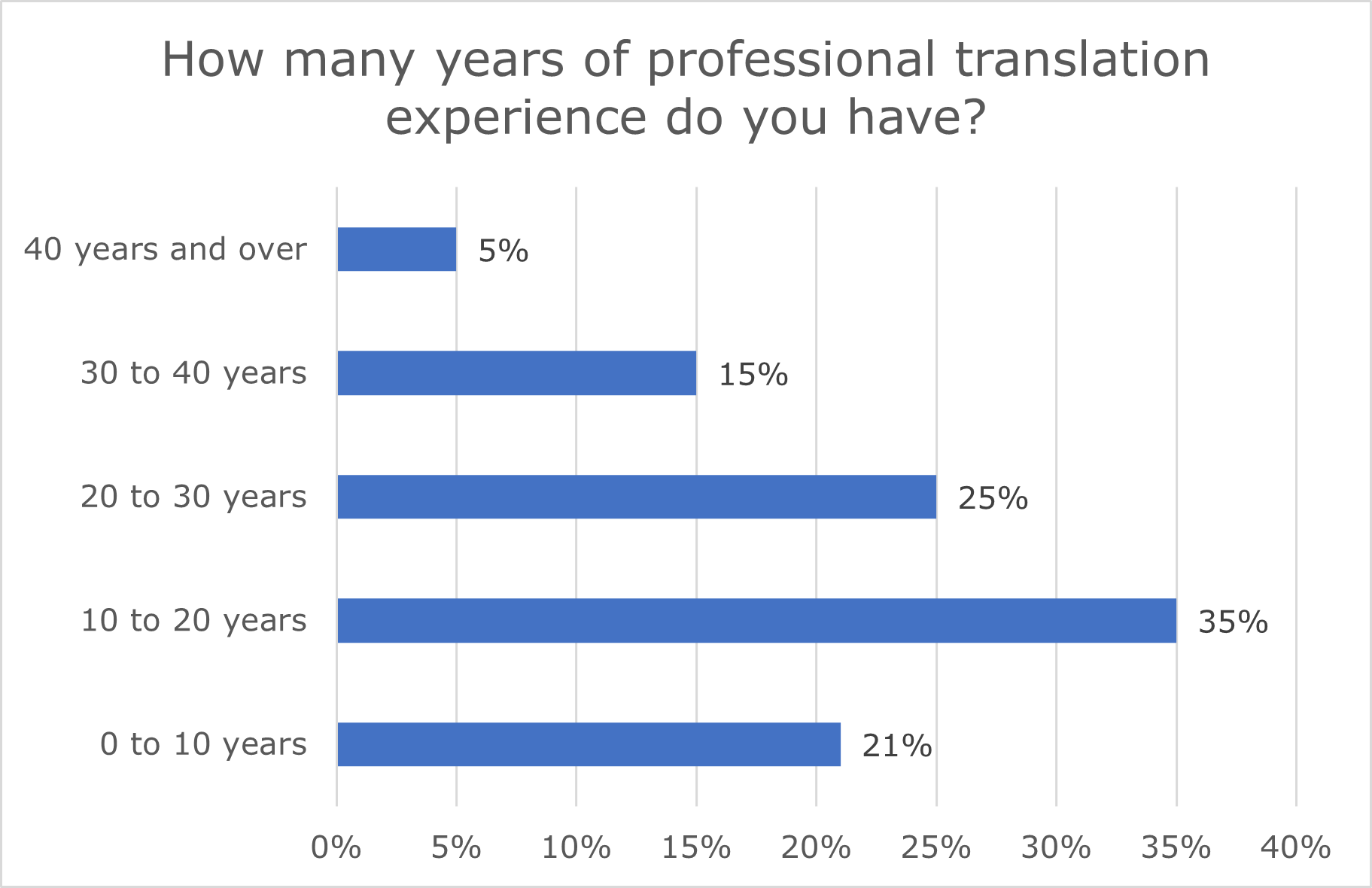
Figure 1. Respondents’ years of professional translation experience.
More respondents were based in the United Kingdom (N=30; 18%) than in any other country, with English<>German, and English<>Spanish as the most common language pairs (Figure 2). There was good international representation: respondents were based in 35 countries across the world (Figure 3) and offered a total of 100 unique language combinations. This distribution, however, was Western-/Eurocentric, with only nine non‑Western countries represented in the survey (N=5 in Latin America, N=2 in the Middle East, N=2 in Africa).
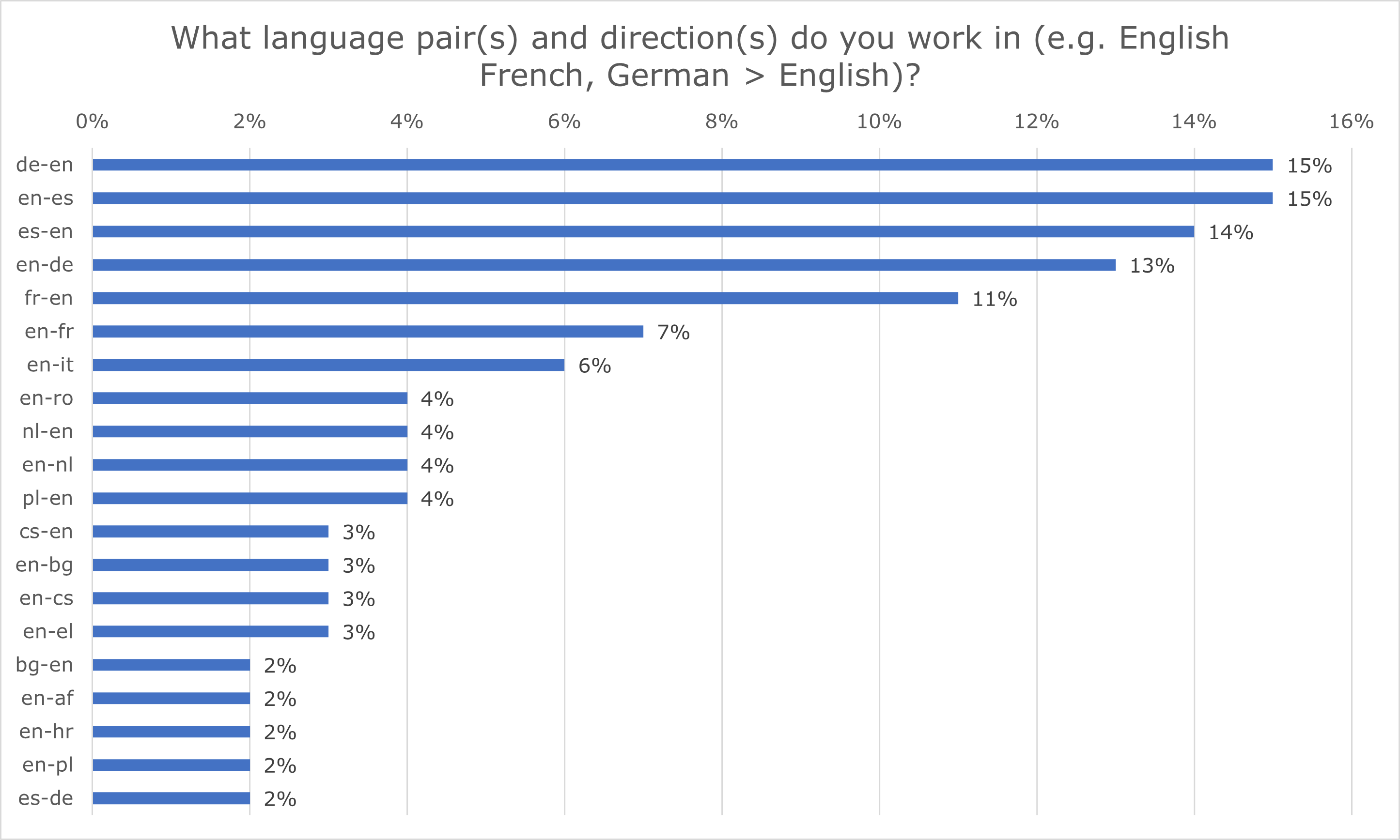
Figure 2. The 20 most frequent language pairs and directions.
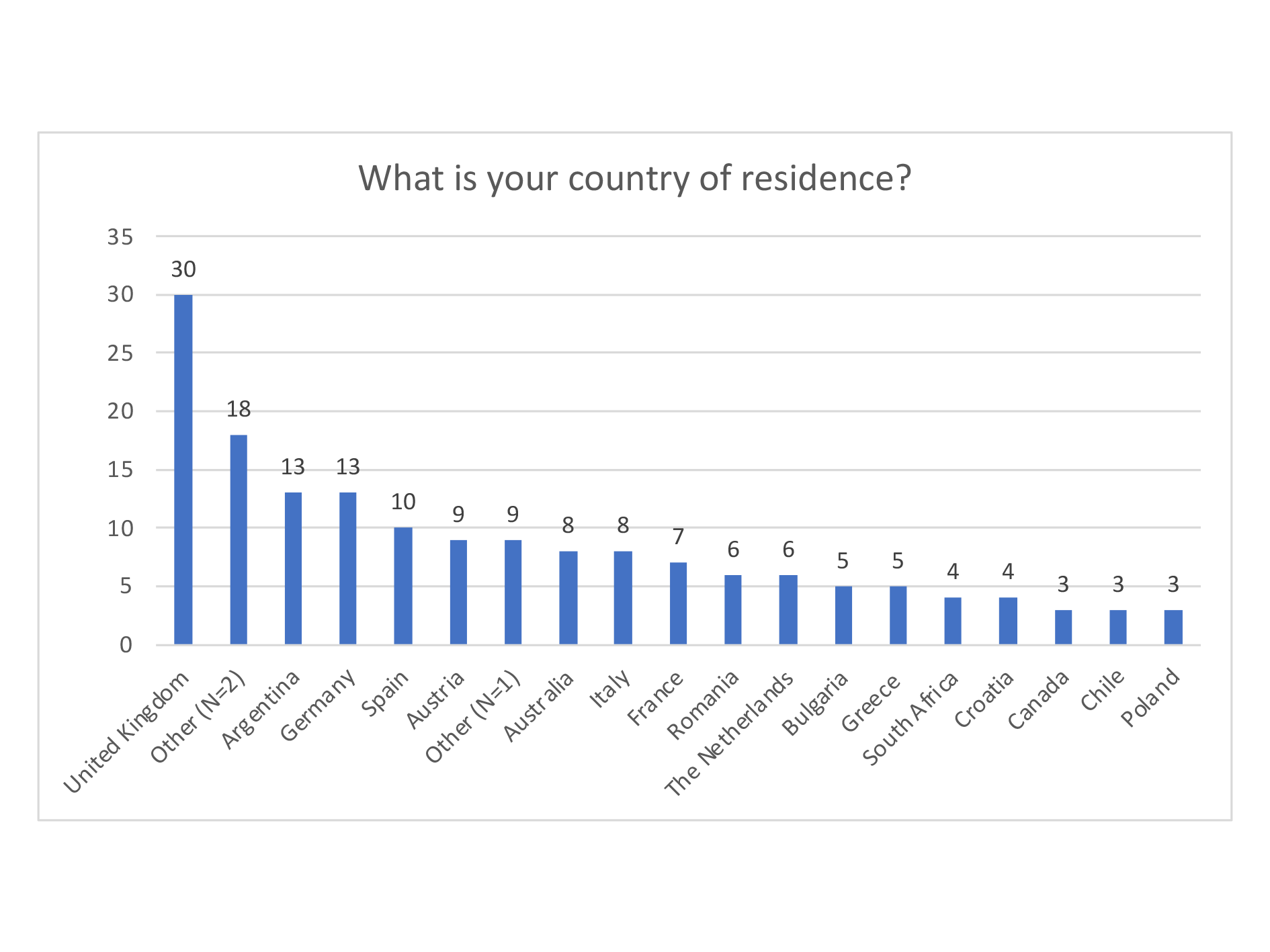
Figure 3. Respondents’ countries of residence.
| What is your country of residence? (cont.) | |
|---|---|
Other (N=2 [each]) |
Belgium, Brazil, Czechia, Estonia, Hungary, Panama, Sweden, Turkey, United States |
Other (N=1 [each]) |
Denmark, Finland, Ireland, Mexico, New Zealand, Portugal, Saudi Arabia, Senegal, Slovakia |
Table 2. Breakdown of respondents’ countries of residence based on
A total of 127 (77%) respondents work as full-time translators, while the remaining 38 have other jobs in addition to translation. A summary of these roles is included in Figure 4. Where respondents mentioned multiple jobs, we only considered the role they listed first in our analysis. Of those with additional roles, most work as interpreters (N=7; 21%), which is a relatively common occurrence in the translation industry (Katan, 2009, p. 191). The six respondents in the ‘Other’ category work in a variety of roles: as an e-learning consultant, homemaker, psychologist, and school director. The remaining two are in the translation industry, one as a part-time freelance medical translator, while the other provides customer support to other freelance translators.
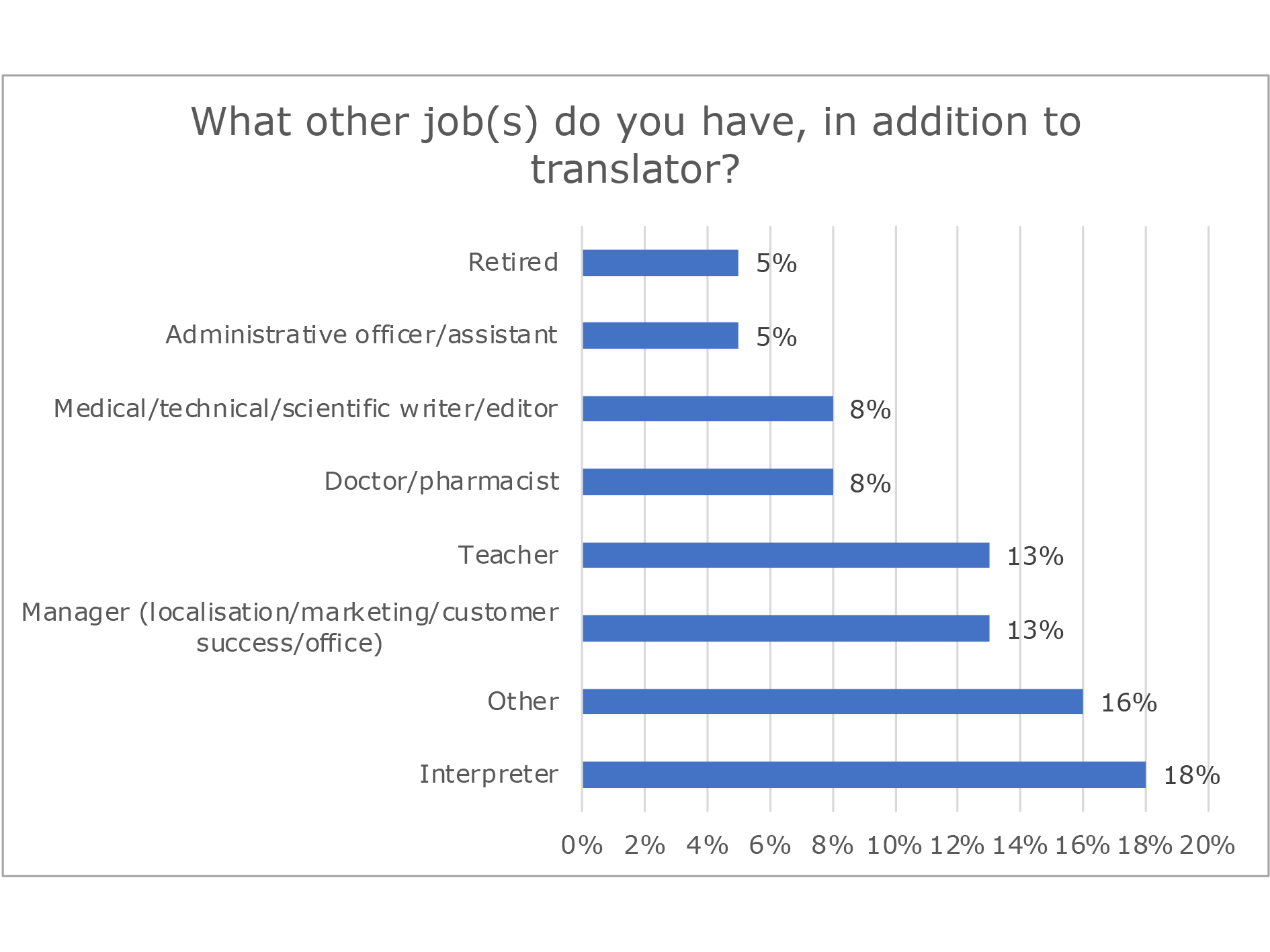
Figure 4. Summary of additional job roles.
An overwhelming majority of respondents (N=156; 95%) work on a self‑employed or freelance basis, whether as translators, revisers, or post‑editors. One respondent provides unpaid or volunteer translation work while working in “customer support in a multinational translation and localization company” (P83). It is unclear whether they perform ad-hoc translation tasks in this role or volunteer as translators in their own time. The remaining sample (N=8; 5%) perform in-house translation tasks, though not necessarily as employed translators: P103 stated they work as a Project Manager, while P29 “translates occasionally for the institution at which [they are] employed, whenever [they are] asked to do so” (the author’s own translation, as this answer was provided in Romanian).
Half of the respondents have academic qualifications and/or professional training in translation, with Figure 5 showing the breakdown of responses by domain. The other respondents fall into two groups: those with training in translation and another field (N=12), which tends to be humanities or science-related (e.g., history, language and literature; biology; medical laboratory diagnostics). Respondents in the second group have backgrounds in other domains (N=25), some of which are translation-adjacent (e.g., interpreting; modern and medieval languages; linguistics), while others are not (e.g., computer science; law and social work; engineering).
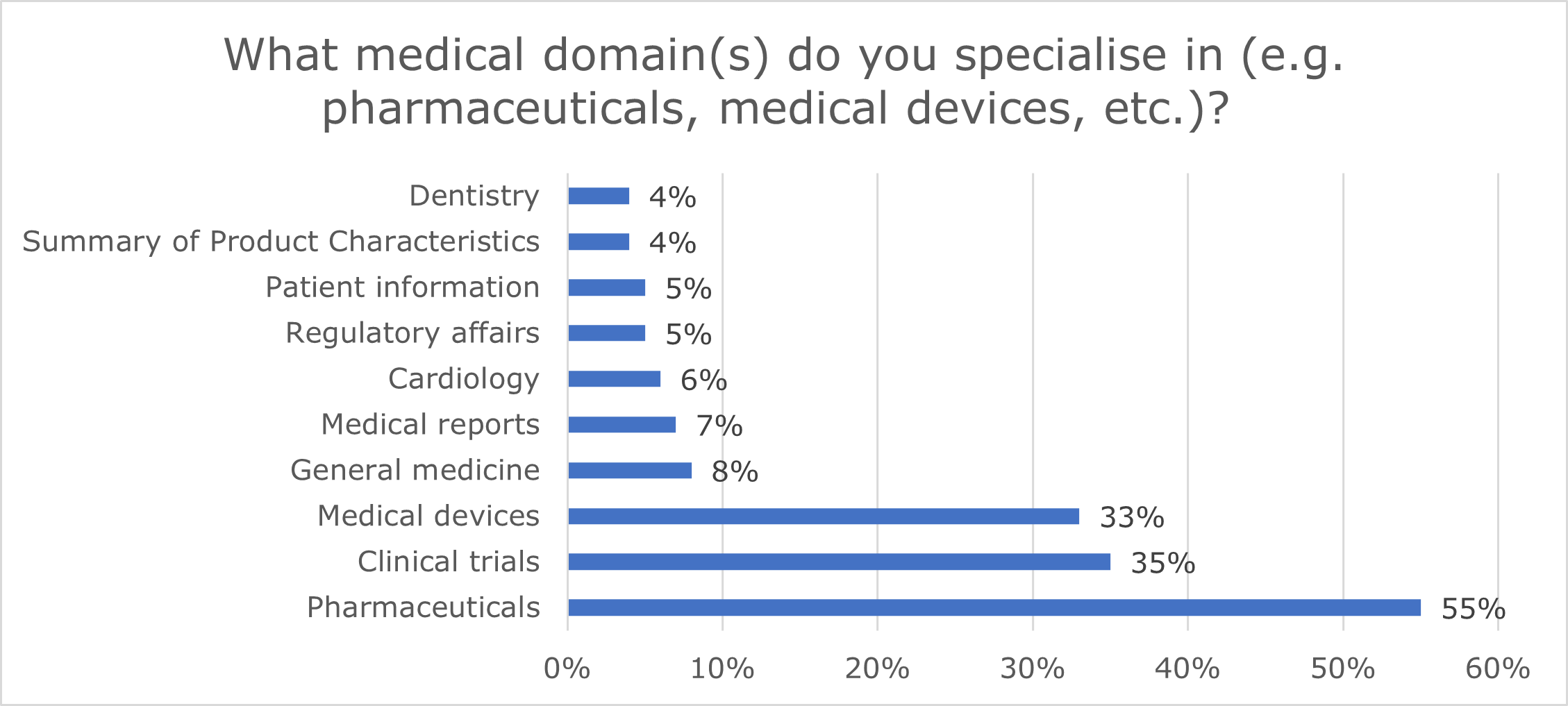 Figure 5. Respondents’ academic qualifications/professional
training.
Figure 5. Respondents’ academic qualifications/professional
training.
4.2 Medical translation work and challenges of translating patient-facing medical texts
In addition to years of translation practice, the survey assessed respondents’ medical translation experience. The mean across the sample was 15.6 years (SD 9.9; median 15), with over a third of respondents having between 10 and 19 years of experience (N=63; 38%, Figure 6). One person reported having 0 years of experience but listed several medical genres they translate, so their answer was considered as valid; they were assigned the least experience in years, compared to 40 years for the most experienced medical translators (N=5).
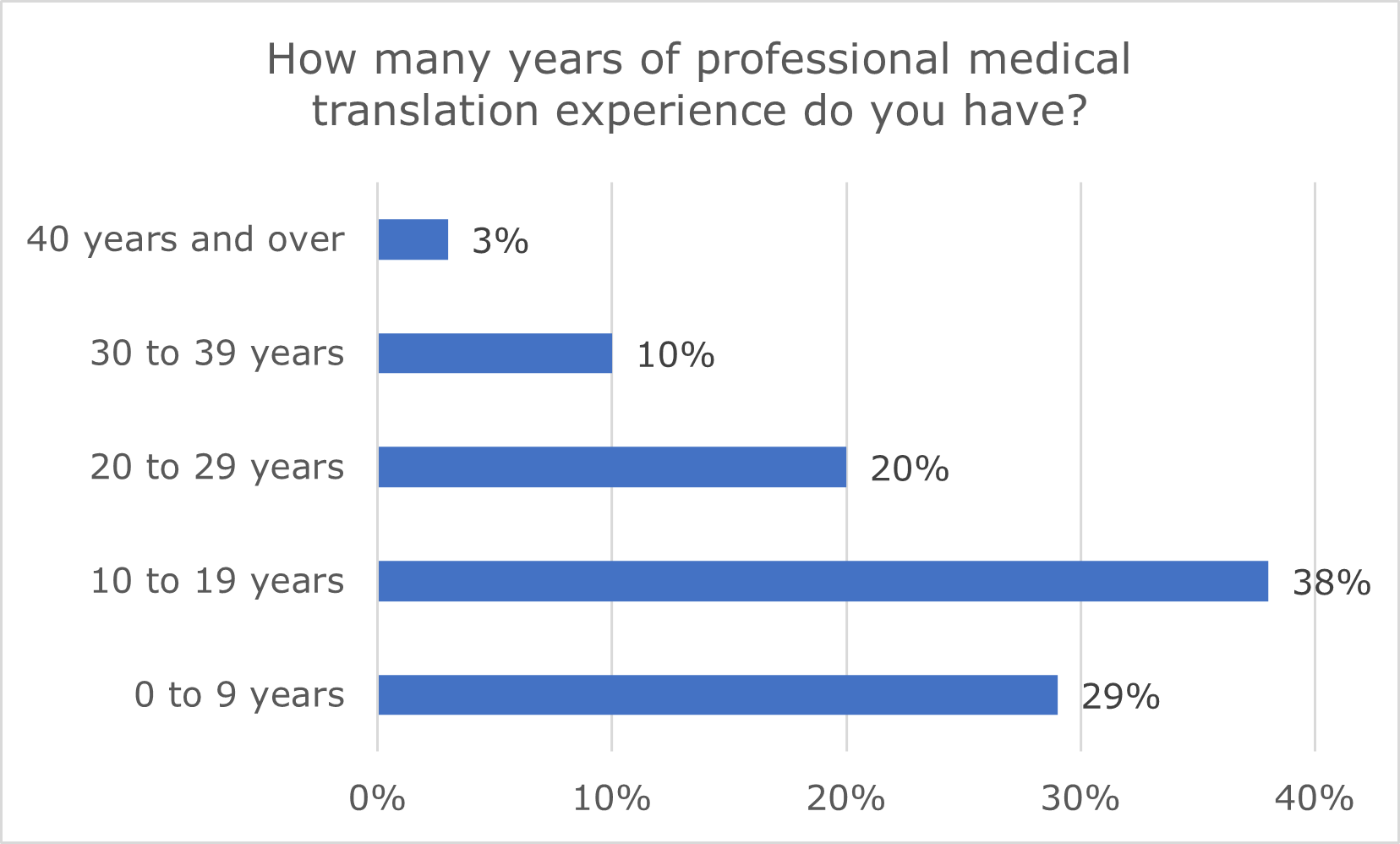
Figure 6. Respondents’ years of professional medical translation experience.
Respondents were asked about their areas of expertise in a free text field; their answers were compiled and grouped by domain. These specialisms were not mutually exclusive, and respondents could input as many as they wished. Figure 7 outlines the ten most common specialisms across the sample.
Figure 7. Respondents’ most common areas of expertise.
Most respondents confirmed they have experience with patient-facing texts such as PILs and ICFs (N=137; 83%), whether as translators, revisers, or post‑editors. This accords with the top three medical domains in Figure 7, which commonly include these text types. These and other texts for patients are highlighted in bold in Table 3.
| Text genre | N | % |
|---|---|---|
| Informed consent forms (ICFs) | 120 | 73% |
| Patient information leaflets (PILs) | 113 | 68% |
| Clinical trial protocols | 100 | 61% |
| Summaries of product characteristics (SmPCs) | 98 | 59% |
| Medical reports | 87 | 53% |
| Instruction manuals | 80 | 48% |
| Clinical trial agreements | 79 | 48% |
| Medical records | 79 | 48% |
| Research articles | 67 | 41% |
| Fact sheets for patients (FSPs) | 66 | 40% |
| Case reports | 65 | 39% |
| Quality of life questionnaires | 63 | 38% |
| Marketing authorisation applications | 53 | 32% |
| Standard operating procedures | 40 | 24% |
| Popular science articles | 37 | 22% |
| Other | 17 | 10% |
| Textbooks | 15 | 9% |
| Patents | 8 | 5% |
Table 3. Text genres translated by the respondents.
Those 137 medical translators with experience in patient-facing texts were asked two follow-up questions on the main text- and process-related challenges in translating these text types. Respondents were asked to rank the challenges listed in decreasing order of difficulty, with an additional ‘Not applicable’ option offered should respondents not want to rank one of the six options provided. This explains why the values in Figures 8 and 9 do not add up to 100%.
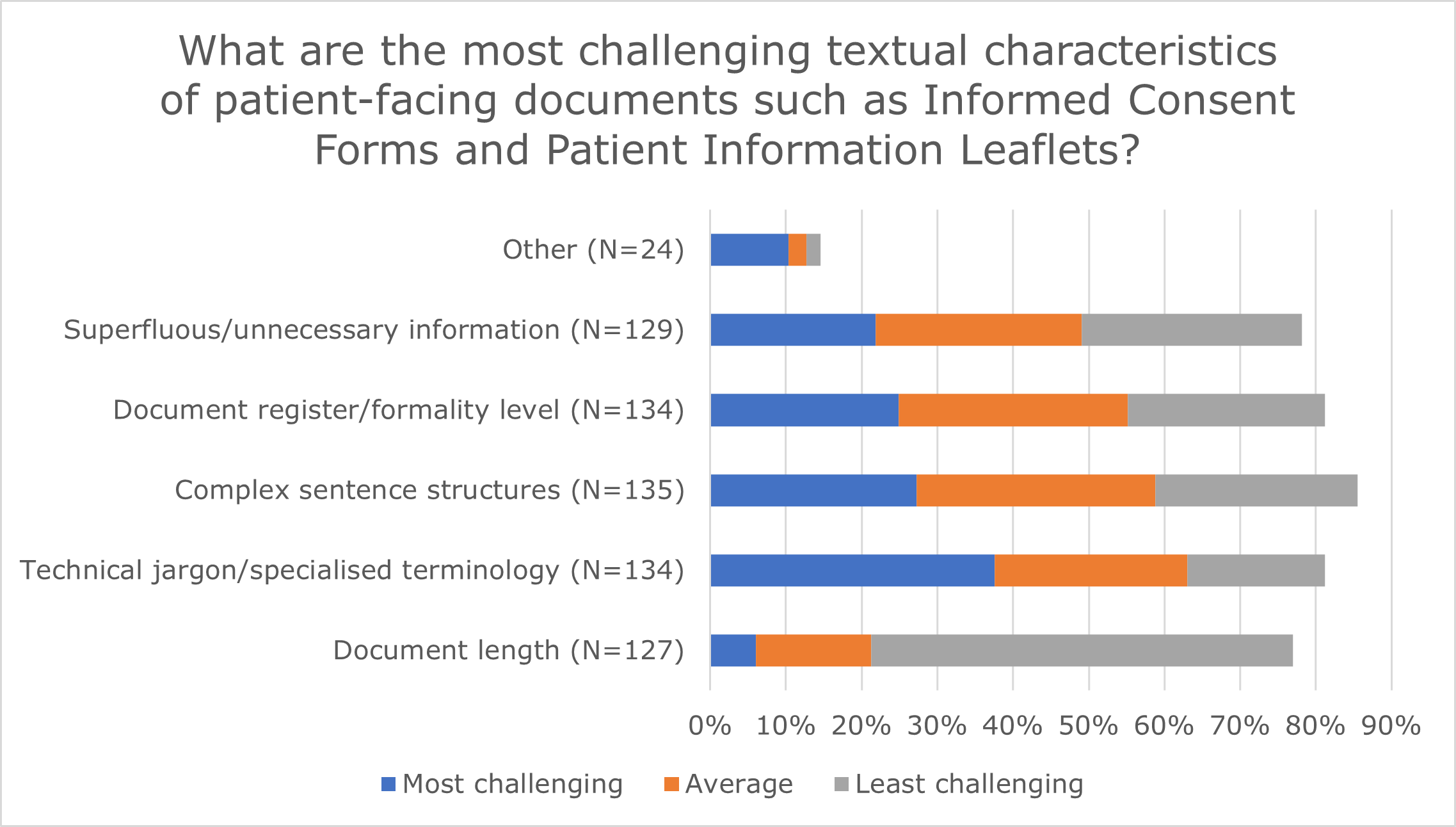
Figure 8. Text-related challenges of translating patient-facing texts.
The first question concerned translation challenges stemming from the text itself, with Figure 8 showing that most challenging was the presence of technical jargon or specialised terminology, according to over a third of respondents (N=62; 38%). Results for the subsequent two challenges tend to be relatively balanced in terms of perceived difficulty, with more respondents rating these as ‘Average’ over the other two levels.
Some respondents listed additional challenges using the ‘Other’ option, most of which were ranked as high in difficulty. These included abbreviations and handwritten information, poorly worded source texts or texts written by non-native speakers, errors and inconsistencies in the source, and gendering in documents pertaining to pregnancy. Template compliance was also referenced; this is addressed under process-related challenges below, so these answers will not be discussed here. Table 4 includes a sample of other self-reported challenges:
| ID | Challenge | Comment |
|---|---|---|
| P4 | Ensuring patient-friendliness | (…) communicating the need to be patient-friendly to clients! |
| P106 | Sometimes finding the most appropriate patient-friendly term. | |
| P110 | Texts by non-natives | The biggest challenge is the translation from English of a text created by [a] non-native author. |
| P53 | Text interventions | Corrections made by the local representatives. These can be often contrary to spelling, grammatical and syntactical target language rules and also to the spirit of the source text. |
| P32 | Gendering | ICFs for pregnant patients and their spouse due to German gender difference. In EN everyone is a patient, but in German it is Patient and Patientin. |
Table 4. Self-reported text-related challenges.
Regarding process-related difficulties, meeting tight deadlines was reported as most challenging (N=65; 39%). Figure 9 shows respondents’ rankings across all six categories listed in the questionnaire.
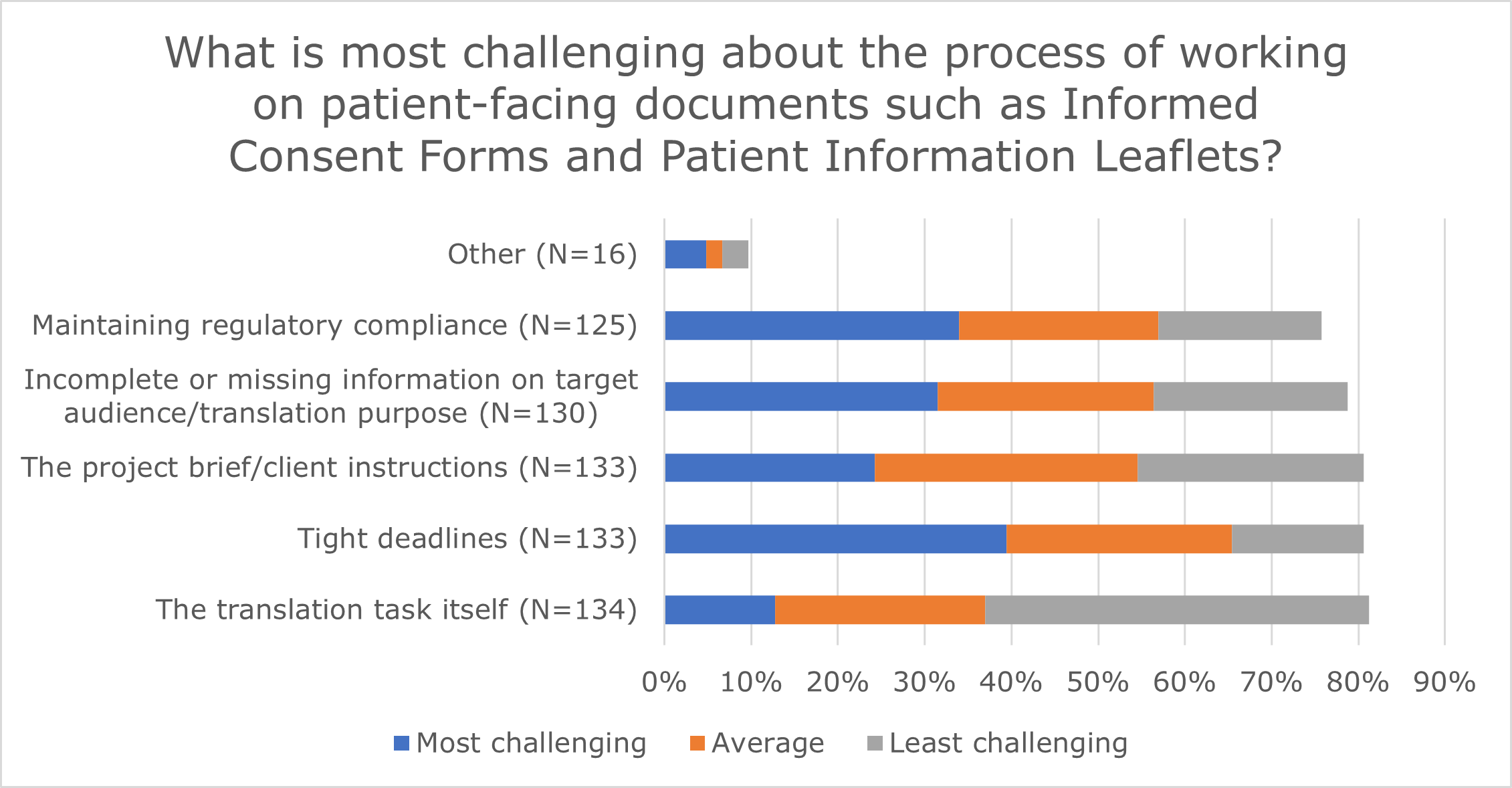
Figure 9. Process-related challenges of translating patient-facing texts.
Of those respondents who selected ‘Other’ (N=16), 12 provided additional information by commenting in the free text field. Some used this option to elaborate on the five challenges listed in the question, while others brought up new issues such as MT and technology. Table 5 presents a sample of their comments:
| ID | Challenge | Comment |
|---|---|---|
| P30 | Technology use | If proofreading/editing, the use of MT for translation usually gives a poorer translation. |
| P131 | The use of CAT tools, often enforced by agencies, makes it difficult to translate as freely as I would like in order to adapt the text to suit the appropriate register/formality. | |
| P90 | The project brief | The project brief can be also very challenging because it is too vague or incomplete (or absent, and one has to keep asking questions). |
| P92 | Lack of consistency Resource access |
Lack of consistency and visibility of local medicine agency rules (not EU directives), issues with paid access to certain databases, rather than being provided with free access |
| P109 | Maintaining compliance | The requirement to stick to the original wording when taking more liberty in wording would render more accurate information and natural-sounding sentences or paragraphs. |
Table 5. Self-reported process-related challenges.
4.3 Usage of CAT tools and speech technologies
The third section of the survey concerns medical translators’ use of translation and speech technologies in their translation and post-editing workflows. Asked how they typically perform translation tasks, most respondents stated they translate in a CAT tool (N=107; 65%), while 48 (29%) work outside CAT tools (e.g., in Microsoft Word or Excel). A further ten respondents chose a third, ‘Other’ option; based on their comments in this free text field, most of them (N=7) work both inside and outside CAT tool environments, with one person specifying that “Outside CAT tools projects [sic] are updates of documents” (P158).
Two-thirds of respondents (N=110; 67%) have post-editing experience and typically perform their post-editing tasks using CAT tools, save for 20 (12%) who post-edit outside CAT tools. Four translators selected the ‘Other’ option. Of these, one person stated they post-edit both inside and outside CAT tools, while the other three commented that they avoid accepting post-editing tasks altogether, despite having experience in the task, as shown in Table 6:
| ID | Post-editing experience | Comment |
|---|---|---|
| P62 | Yes | I avoid accepting such jobs |
| P92 | Yes | I have experience, but I refuse to accept PE tasks in this field |
| P105 | Yes | I have very limited experience and have given up on MTPE. It is an absolute nightmare and totally unrewarding in every respect. |
Table 6. Self-reported post-editing uptake.
Only 15% (N=24) of respondents reported having used ASR tools to dictate their translations, whether in the medical domain or other specialisms (Table 7). Possible reasons for this low uptake are discussed in Section 5. Of these, almost all (N=23) had used Dragon Naturally Speaking,4 with one translator mentioning Hey memoQ.5 Figure 10 shows how often respondents use ASR to dictate their translations; most (N=14; 58%) use it occasionally, depending on task and text type.
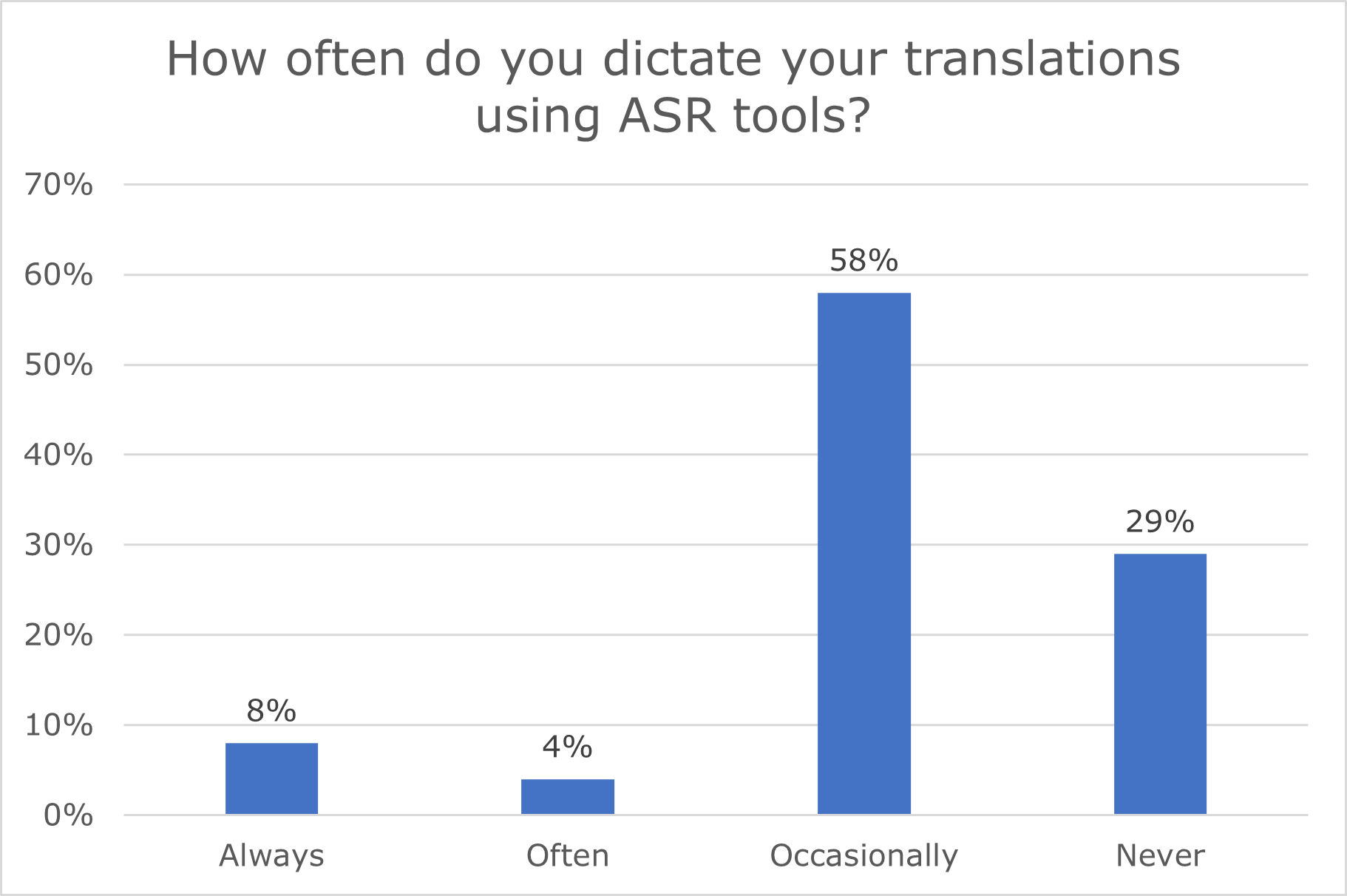
Figure 10. Frequency of ASR use for translation dictation (N=24).
Respondents mentioned using ASR to dictate various text types and projects, which can broadly be grouped into themes (Table 7):
| Text type | N | % |
|---|---|---|
| Specialised (medical/legal/technical) | 6 | 25% |
| No text types | 6 | 25% |
| General/non-technical | 5 | 21% |
| Marketing/editorial | 4 | 17% |
| All text types | 3 | 13% |
Table 7. Text types translated using ASR dictation.
Respondents gave several reasons for choosing to dictate their translations instead of typing them: most use ASR for health-related reasons to avoid strain on their muscles and joints (N=13; 54%), while a third (N=8; 33%) use it to speed up their work. A small proportion (N=4; 17%) mentioned that dictating their translations helps improve the fluency of their output, as shown in Table 8:
| ID | Comment |
|---|---|
| P4 | But with spoken text (videos) it's great to achieve a lovely and natural flow |
| P111 | It allows me to hear how the translation sounds as I'm listening to myself dictate. |
| P156 | More fluent, faster |
Table 8. Self-reported motivations for using ASR dictation.
Of interest was also whether respondents’ attitudes and working practices had changed since using ASR to dictate their translations. For six respondents, the change was for the worse, despite their initial willingness to try out ASR tools. Three respondents noted a positive change. A sample of their comments is provided in Table 9:
| ID | Type of change | Comment |
|---|---|---|
| P1 | Negative | Now use ASR less than previously due to increase in post-editing MT, as effort to edit in a CAT tool too great |
| P51 | Negative | Have adapted it to use with SDL Trados which can be very cumbersome and only works up to a certain extent. I tend to use it less now than initially. |
| P146 | Negative | I used it a lot at the beginning, however using it within translation tools like Trados, poses a number of problems, like slow, unexpected crashes, limited functionality, and so it depends a lot on the type of text whether it actually is effective. I tend to use it a more when there is a lot of translation to do, for health reasons, but with normal work loads, I now hardly use it. |
| P32 | Positive | I noticed that my translations became more natural sounding, more like spoken language. Maybe because I was not typing in CAT segmented text but the tool was doing it for me. I still prefer typing though. |
| P78 | Positive | Yes. At first I didn't like it and only used it on more urgent projects. Now it's become my default way of working. |
| P160 | Positive | I wish I had used it earlier |
Table 9. Self-reported changes in attitude and working practices after using ASR.
Finally, all respondents were asked to rank their preferred way of working (i.e., typed translation from scratch, post-editing or dictated translation using ASR tools) in decreasing order of preference. Figure 11 shows that an overwhelming majority of respondents (N=137; 83%) favour traditional typed translation, with post-editing as the second option at a considerable distance (N=55; 33%). Dictated translation using ASR tools ranks as respondents’ least preferred way of working (N=48; 29%), though this is likely due to the limited numbers of respondents who have experience using these tools.
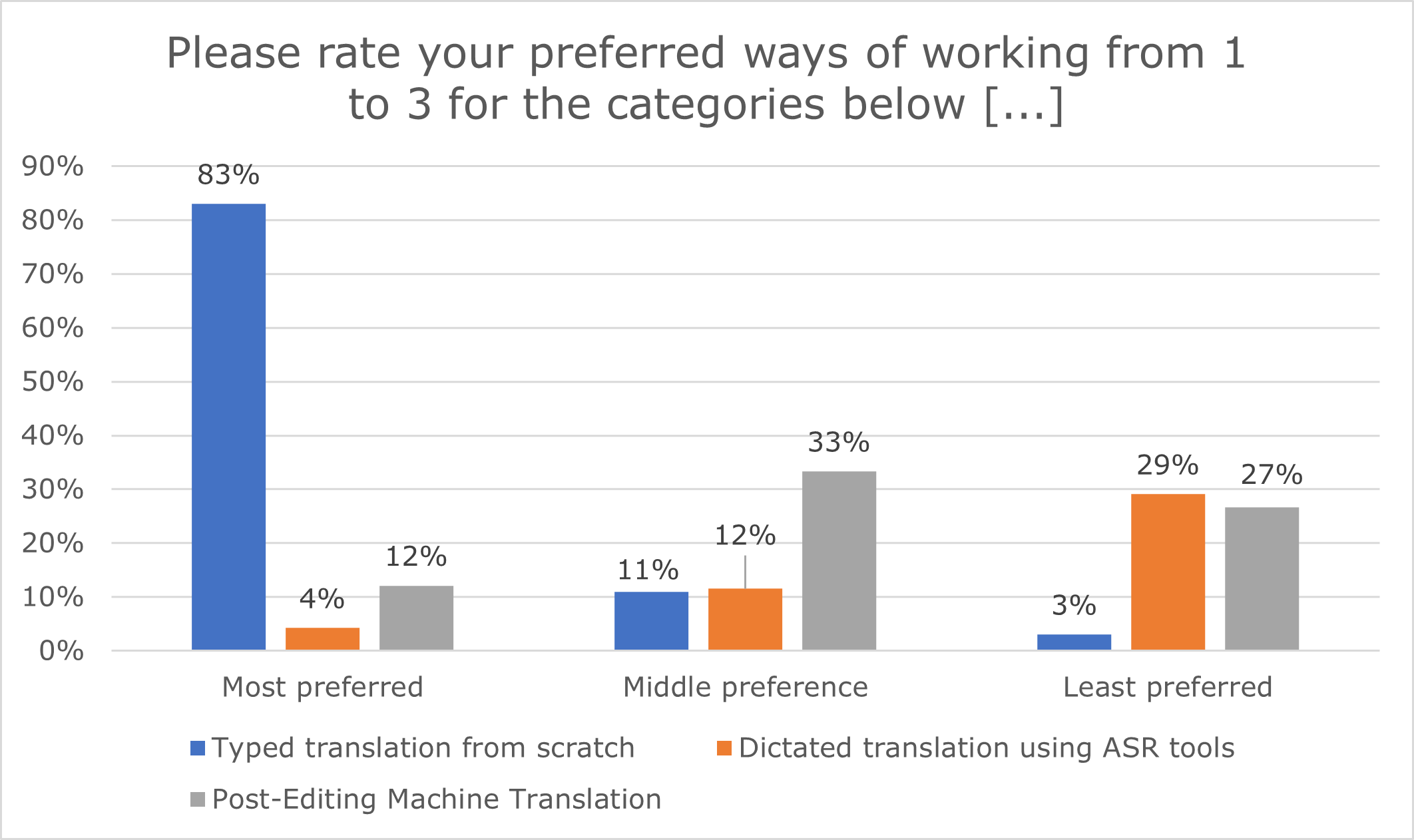
Figure 11. Respondents’ preferred way of working.
5. Discussion
Based on these results, we can identify certain trends in the respondents’ profiles and practices, which allow us to address our three research questions. It is worth noting at this point that this survey does not aim to be representative of the entire population of professional medical translators given its limited sample size, the socio-demographic and professional coverage of the respondents and the snowball sampling technique used for dissemination. Rather, this work is exploratory and interpretative in nature. We hope that the findings may highlight existing trends in the professional reality of medical translators, and further debates and research on their current and future practices (Alonso, 2015, p. 93; Muñoz-Miquel et al., 2020, p. 151).
In response to RQ1, we see that medical translation is predominantly female-centric. Although some evidence suggests women tend to respond to surveys more than men (Smith, 2008), our results reflect trends in the wider translation industry (Pym et al., 2012; Alonso, 2015; ELIA et al., 2023) and in similar studies on Spanish- and French-speaking medical translators (Muñoz-Miquel, 2018; Muñoz-Miquel et al., 2020; Vidrequin, 2022). While English-Spanish and, to a lesser extent, English-French were better represented in our survey compared to other language pairs (15% and 7% respectively), it is unclear whether these similarities result from this distribution, especially since German-English is tied with English-Spanish as the most common language pair among our respondents.
Medical translators tend to be in their early or late middle age and have considerable professional translation experience, which in our case was 20 years, on average. The finding that they primarily work as freelancers is consistent with industry trends (Katan, 2009; Pym et al., 2012), but their full‑time employment status is not. It is possible that distributing our survey via professional translator associations, among other methods, may have shaped this result, as full-time translators are potentially more likely to be members of such associations and receive newsletters and promotional communications. When respondents have additional jobs, these are usually translation- or medicine-adjacent, with translation and interpreting being a common pairing.
Most medical translators have academic qualifications or professional training, which shows a high degree of specialisation across the group. A background in translation, whether as a standalone subject or in conjunction with other domains, remains the most common entry point to medical translation, rather than training in medicine/science, which suggests that for this latter group, the “translation profession [might not be a] natural career” (Muñoz-Miquel, 2018, p. 25). While these results mirror findings in Muñoz-Miquel (2018) and Martínez (2019) on Spanish and Spanish/French medical translators, our survey dissemination methods may have favoured “the academically trained translators” (Katan, 2009, p. 201) due to the author’s professional network. Likewise, the preponderance of respondents with training in translation over other fields may again be an effect of their being members of professional translation associations. However, these trained translators accounted for only half of all respondents, and there were other backgrounds represented in the survey.
The levels of experience and expertise seen among respondents serve as the required barriers to entry for what is necessarily a high-risk, zero-error domain, with stringent quality requirements and task complexity. In her study, Martínez (2019) claimed there is a correlation between years of experience and the volume of medical translation work performed, with professional practice evolving in a way which requires increasing specialisation (ibid., p. 316). This could explain the predominance of full-time freelancers among our survey respondents and highlight the need for continuous specialised training throughout medical translators’ careers.
Regarding RQ2, results confirm that most medical translators work on patient-facing texts such as PILs and ICFs as part of their standard service provision, particularly in the pharmaceutical and clinical research fields. This reflects the growing importance of patient-centredness in healthcare. As expected, translating specialised terminology and jargon is the greatest text-related challenge to medical translators. Given the high level of experience and expertise across our respondents, this challenge is likely compounded by having to adapt to the needs and expectations of laypersons and sourcing “the most appropriate patient-friendly term” (P106), rather than having to do with translators’ in-domain knowledge or research skills.
The finding that terminology is a major concern is also reflected in research, which suggests that “there is a tendency to revert to expert medical language” among medical translators when working on patient-facing texts (Montalt et al., 2018, p. 34), resulting in translations which “fail to reach the layman target group by failing to carry out the intralingual part of the translation” (ibid.). Medical translators may resort to different strategies to overcome these challenges (“I always aim to reduce the complexity of sentences where appropriate and use less technical terms”, P144), but the regulatory conventions and constraints governing translations of medical texts for patients limit the extent of possible intervention (“the requirement to stick to the original wording when taking more liberty in wording would render more accurate information and natural-sounding sentences or paragraphs”, P109).
The other text-based challenges also highlight the incompatibility between texts for medical experts and those for patients or other laypersons. Complex sentences, a formal register and exhaustive detailing are closely related linguistic phenomena typical of high-level medical communication where accuracy and comprehensiveness are essential. They may not, however, be appropriate for the general population, whose information needs require clarity and comprehensibility. These challenges likely stem from the way in which these texts are written (“I wish I could completely rewrite badly-written source texts”, P127), which in turn impacts the translation product and process.
Tight delivery deadlines pose the biggest process-related challenge for medical translators, though this is indicative of wider trends in the translation industry. While regulatory compliance and insufficient information on the target audience or translation purpose are not specific to the medical domain, they highlight the working reality of the many medical translators who are required to perform increasingly specialised tasks (e.g., following EMA templates and procedures) without sufficient knowledge of the context. This renders the translation process even more difficult, particularly in a patient-centred setting, as translators may be unaware of the type of intralingual or intergeneric adaptation required. As is the case in many other translation specialisms, this puts the onus on translators to actively seek out the missing information either through research or by asking the client (“the project brief […] is too vague or incomplete (or absent, and one has to keep asking questions)”, P90).
In response to RQ3, results show that medical translation is a ‘technologised’ profession (Moorkens, 2017). CAT tools are widely used for both translation and post-editing, with only a limited number of respondents performing tasks outside of these environments (such as document updates). Acceptance and experience of post-editing appear relatively high, compared to rates identified in similar studies on French (51% in Vidrequin, 2022: 255) and Spanish-speaking medical translators (44% in Muñoz-Miquel et al., 2020, p. 147). Since a considerable proportion of our respondents also work in these language combinations, it is unclear what causes this difference, whether variations in the quality of MT engine performance or a pushback against post-editing itself.
Medical translators have considerably less experience using ASR in their translation workflows. There might be several reasons for low ASR usage among our respondents, from a preference for typed translation, to not having their languages supported by speech recognition tools. Difficulty integrating with CAT tools could be another factor, as reported by one of the respondents in relation to Dragon Naturally Speaking, the most commonly used ASR tool among our respondents: “Have adapted it to use with SDL Trados which can be very cumbersome and only works up to a certain extent. I tend to use it less now than initially” (P51).
This lack of support and flexibility may be why ASR tools are not more widely used in medical translation, rather than translators’ openness or the tools’ usability for specific text types. Those medical translators who have integrated ASR into their practice reported using it for a variety of tasks and text types, from the highly specialised, to the more general. Some of those who were not put off by technology-related challenges also reported their opinions of ASR changing for the better after trying it out, with one translator turning to dictation as their default way of working. Though limited, results also suggest that dictating one’s translations may have a positive impact on the fluency and naturalness of the translated output (Table 8), bringing it closer to spoken communication, in keeping with findings by Ciobanu (2016). This could have important applications in patient-facing medical translations, potentially serving to mitigate some of the challenges inherent in the genre, as discussed in Section 4.2.
6. Limitations
Our findings are not generalisable or representative of medical translators at large due to the sample size and the snowball sampling used to disseminate the survey. This technique carries the risk of sampling bias, which could have influenced results such as the preponderance of respondents trained in translation, or their status as full-time freelancers given the survey distribution via professional translator associations. To broaden the reach of the survey beyond these groups, the author drew on their professional network, which includes representatives from pharmaceutical companies and clinical research organisations. However, their response was limited, and further dissemination was not reached via these channels.
Although the survey targeted medical translators from across the globe, respondents’ distribution is heavily Western/Eurocentric. While the author contacted several non-Western translator associations (e.g., in Chile, South Africa and Japan), non-Western translators are poorly represented in the survey. This is likely an effect of the author’s Western-based professional network, their limited access to non-Western dissemination channels, as well as the questionnaire only being offered in English. This may have prevented non-English speakers or translators without English as a working language from participating in the survey. Despite these limitations, we hope the variety and number of responses received in this exploratory study have helped highlight certain trends and allowed us to contribute to existing research in the medical translation profession.
A final limitation is inherent in the use of surveys without other research methods. Surveys mainly rely on respondents’ self-reported data, which is subjective and vulnerable to recall bias. They may only reflect respondents’ perceptions at a moment in time (e.g., particular translation challenges), and are not the best instruments to collect explanatory data unless accompanied by other methods (Saldanha & O’Brien, 2013, p. 152). Overcoming this limitation requires a mixed-methods research approach, whereby qualitative and quantitative data are triangulated for more robust results; this approach is used in the author’s doctoral project, which includes the present survey, as well as a corpus linguistics analysis and an eye-tracking study.
7. Conclusion and Future Work
This paper has provided an overview of professional medical translation based on findings from an international survey on 165 medical translators.
Medical translators work in fast-paced and highly specialised environments where requirements for quality go beyond the source text to reflect developments within healthcare and the wider medical industry. The variety of medical genres, increased task complexity, and rising expectations for faster deliveries driven by CAT and MT usage, all reflect the working reality of professional medical translators. Coping with these demands requires considerable experience and expertise, both linguistic and domain-related, which explains the high degree of training and specialisation seen across our respondents, along with the longevity of their careers.
Expertise is paramount in medical translations for patients and other laypersons. Beyond the interlinguistic transfer required, these translations entail intralingual adaptation between the expert and lay contexts, with medical translators often serving as mediators between the two. Perhaps this explains why respondents found terminology-related challenges as most difficult, since technical jargon requires specific mitigation strategies in texts for lay target audiences. This is further complicated by process-related challenges, with medical translators required to follow established regulatory templates, while also working with insufficient information on the purpose of the translation or the intended target audience.
Finally, while CAT tools are widely used in medical translation in a variety of workflows, there may be untapped potential concerning ASR, particularly in patient-facing translations. This is reflected in some interest from medical translators, although limited software offerings may hinder their wider use, at least at present. The productivity and fluency improvements reported by some ASR users point to a useful avenue of research, especially with reference to comparative investigations against MT and CAT tools. The author’s doctoral work will assess the impact of these three tools on medical translators’ output and workflows, in terms of productivity, cognitive load, output quality, and attitudes.
Future research could explore other medical text genres, which would provide additional insights into broader product and process-related challenges encountered by medical translators, as would comparative studies between translation issues in texts for medical experts and those for laypersons. The scope of technology-related investigations could also be expanded by addressing potential applications of generative AI in medical translation tasks, particularly in patient-facing contexts, given its capabilities to simplify and/or synthetise complex information.
Acknowledgements
The author wishes to thank all the translators who took part in the survey, those who assisted with reviewing, piloting, and identifying distribution channels for the questionnaire, as well as the colleagues, contacts and professional translator associations who agreed to disseminate it.
References
Alonso, E. (2015). Analysing the use and perception of Wikipedia in the professional context of translation. The Journal of Specialised Translation, 23, 89–116.
Bolaños-Medina, A. (2012). The key role of the translation of clinical trial protocols in the university training of medical translators. The Journal of Specialised Translation, 17, 17–36.
Buysschaert, J. (2021). Medical terminology and discourse. In Ş. Susam-Saraeva & E. Spišiaková (Eds.). The Routledge Handbook of Translation and Health (1st ed.) (pp. 65–79). Routledge.
Cadwell, P., O’Brien, S. & Teixeira, C.S. (2018). Resistance and accommodation: factors for the (non-) adoption of machine translation among professional translators. Perspectives, 26(3), 301–321. https://doi.org/10.1080/0907676X.2017.1337210
Ciobanu, D. (2016). Automatic Speech Recognition in the professional translation process. Translation Spaces, 5(1), 124–144. https://doi.org/10.1075/ts.5.1.07cio
Ciobanu, D. & Secară, A. (2019). Speech recognition and synthesis technologies in the translation workflow. In M. O’Hagan (Ed.). The Routledge Handbook of Translation and Technology (1st ed.) (pp. 91–106). Routledge.
CIOL & ITI (2011). 2011 Rates and Salaries Survey for Translators and Interpreters. Chartered Institute of Linguists and Institute of Translation and Interpreting. https://docplayer.net/14742908-2011-rates-and-salaries-survey-for-translators-and-interpreters.html
Ehrensberger-Dow, M. & O’Brien, S. (2015). Ergonomics of the Translation Workplace: Potential for Cognitive Friction. Translation Spaces, 4(1), 98–118. https://doi.org/10.1075/ts.4.1.05ehr
ELIA, EMT, EUATC, FIT EUROPE, GALA, LIND & Women in Localization (2023). 2023 European Language Industry Survey. Trends, expectations and concerns of the European language industry. https://elis-survey.org/wp-content/uploads/2023/03/ELIS-2023-report.pdf
Ezpeleta Piorno, P. (2021). An example of genre shift in the medicinal product information genre system. Linguistica Antverpiensia, New Series – Themes in Translation Studies, 11, 168–187.
Farrell, M. (2023). Do translators use machine translation and if so, how? Results of a survey among professional translators. In J. Moorkens & V. Sosoni (Eds.). Proceedings of the 44th Translating and the Computer (TC44) conference (pp. 49–60). Tradulex.
Gamal, S. (2020). The Memory of Knowledge: An Analytical Study on Translators’ Perceptions and Assessment of CAT Tools with Regard to Text Genre. International Journal of Linguistics and Translation Studies, 1(2), 1–18. https://doi.org/10.36892/ijlts.v1i2.47
Gaspari, F., Almaghout, H. & Doherty, S. (2015). A survey of machine translation competences: Insights for translation technology educators and practitioners. Perspectives, 23(3), 333–358. https://doi.org/10.1080/0907676X.2014.979842
Hickey, S. (2023). Nimdzi 100 2022: Ranking of Top Language Service Companies, Nimdzi. https://www.nimdzi.com/nimdzi-100-top-lsp/
Jiménez-Crespo, M. Á. & Tercedor Sánchez, M. (2017). Lexical variation, register and explicitation in medical translation: A comparable corpus study of medical terminology in US websites translated into Spanish. Translation and Interpreting Studies, 12(3), 405–426. https://doi.org/10.1075/tis.12.3.03jim
Katan, D. (2009). Occupation or profession: a survey of the translators’ world. The Journal of the American Translation and Interpreting Studies Association, 4 (2), 187–209. https://doi.org/10.1075/tis.4.2.04kat
Karwacka, W. (2021). Quality, accessibility and readability in medical translation. In Ş. Susam-Saraeva & E. Spišiaková (Eds.). The Routledge Handbook of Translation and Health (1st ed.) (pp. 80–95). Routledge.
Krüger, R. (2023). Artificial intelligence literacy for the language industry – with particular emphasis on recent large language models such as GPT-4. Lebende Sprachen, 68(2), 282–330. https://doi.org/10.1515/les-2023-0024
Liyanapathirana, J. & Bouillon, P. (2022). Integrating post-editing with Dragon speech recognizer: a use case in an international organization. In J. Esteves-Ferreira et al. (Eds.). Proceedings of the 43rd Translating and the Computer (TC43) conference (pp. 55–67). Tradulex.
Maeda-Nye, M. (2009). The importance of translation in clinical trials. https://www.tjc-global.com/the_importance_of_translation_in_clinical_trials/.
Martínez, L. (2019). L'impact de la technologie sur les traductions spécialisées. Le cas de la traduction médicale. Des mots aux actes, 8, 309–326. https://doi.org/10.15122/isbn.978-2-406-09779-2.p.0309
Montalt, V., Zethsen, K. K., & Karwacka, W. (2018). Medical translation in the 21st century - challenges and trends. MonTI. Monografías de Traducción e Interpretación, 10, 27–42. https://www.e-revistes.uji.es/index.php/monti/article/view/3684
Montalt-Resurrecció, V. & Shuttleworth, M. (2012). Research in translation and knowledge mediation in medical and healthcare settings. Linguistica Antverpiensia, New Series – Themes in Translation Studies, 11, 9–29. https://doi.org/10.52034/lanstts.v11i.294
Moorkens, J. (2017). Under pressure: translation in times of austerity. Perspectives, 25(3), 464–477. https://doi.org/10.1080/0907676X.2017.1285331
Muñoz Martín, R. (2014). Situating Translation Expertise: A Review with a Sketch of a Construct. In J.W. Schwieter & A. Ferreira (Eds.). The Development of Translation Competence: Theories and Methodologies from Psycholinguistics and Cognitive Science (pp. 2–56). Cambridge Scholars.
Muñoz-Miquel, A. (2018). Differences between linguists and subject-matter experts in the medical translation practice: An empirical descriptive study with professional translators. Target, 30(1), 24–52. https://doi.org/10.1075/target.14130.mun
Muñoz-Miquel, A., Montalt, V., & García-Izquierdo, I. (2020). Fostering Employability through Versatility within Specialisation in Medical Translation Education. HERMES - Journal of Language and Communication in Business, 60, 141–154. https://doi.org/10.7146/hjlcb.v60i0.121316
Nisbeth Brøgger, M. (2017). When Translation Competence Is Not Enough: A Focus Group Study of Medical Translators. Meta, 62(2), 396–414. https://doi.org/10.7202/1041030ar
Nisbeth Brøgger, M. & Zethsen, K. K. (2021). Inter- and intralingual translation of medical information: The importance of comprehensibility. In Ş. Susam-Saraeva & E. Spišiaková (Eds.). The Routledge Handbook of Translation and Health (1st ed.) (pp. 96–107). Routledge.
Nisbeth Jensen, M. & Zethsen, K. K. (2012). Translation of patient information leaflets: Trained translators and pharmacists-cum-translators – a comparison. Linguistica Antverpiensia, New Series – Themes in Translation Studies, 11, 31–49. https://doi.org/10.52034/lanstts.v11i.295
O’Brien, S. & Conlan, O. (2018). Moving Towards Personalising Translation Technology. In H. V. Dam, M. Nisbeth Brøgger, & K. Korning (Eds.). Moving Boundaries in Translation Studies (pp. 81–97). Routledge.
Pilegaard, M. & Ravn H. B. (2013). Informed consent: towards improved lay-friendliness of patient information sheets. Communication & Medicine, 10(3), 201–211. https://doi.org/10.1558/cam.v10i3.201
Pym, Anthony et al. (2012). The Status of the Translation Profession in the European Union: Final Report. Publications Office of the European Union. https://data.europa.eu/doi/10.2782/63429
Ruokonen, M. & Mäkisalo, J. (2018). Middling-status profession, high-status work: Finnish translators’ status perceptions in the light of their backgrounds, working conditions and job satisfaction. Translation & Interpreting, 10(1), 1–17. https://doi.org/10.12807/ti.110201.2018.a01
Saldanha, G. & O’Brien, S. (2013). Research methodologies in translation studies (1st ed.). Routledge.
Sand, K., Eik-Nes, N. L., & Loge, J. H. (2012). Readability of informed consent documents (1987-2007) for clinical trials: a linguistic analysis. Journal of Empirical Research on Human Research Ethics: JERHRE, 7(4), 67–78. https://doi.org/10.1525/jer.2012.7.4.67.
Simonsen, H. K. (2014). Danglers in patient information leaflets and technical manuals: an issue for specialised translators? The Journal of Specialised Translation, 21, 2–18.
Smith, G. (2008). Does gender influence online survey participation? A record-linkage analysis of university faculty online survey response behavior. ERIC Document Reproduction Service No. ED 501717.
Stokes, K. (2022). CIOL Insights: The Languages Professions II. Chartered Institute of Linguists. https://www.ciol.org.uk/ciol-insights-languages-professions-2.
Verplaetse, H. & Lambrechts, A. (2019). Surveying the use of CAT tools, terminology management systems and corpora among professional translators: General state of the art and adoption of corpus support by translator profile. Parallèles, 31(2), 3–31. https://doi.org/10.17462/para.2019.02.01
Vidrequin, M. (2022). Assessing Quality and Use of MT by Professional Freelance Translators in the Medical Field. In S. Castilho et al. (Eds.). Proceedings of the New Trends in Translation and Technology Conference - NETTT 2022 (pp. 254–258). https://acl-bg.org/proceedings/2022/NeTTT%202022/NeTTT-2022-Final-Proceedings.pdf#chapter.31
Zapata, J., Castilho, S., & Moorkens, J. (2017). Translation dictation vs. post-editing with cloud-based voice recognition: a pilot experiment. In M. Yamada & M. Seligman (Eds.). Proceedings of MT Summit XVI (pp. 116–129). MT Summit.
Zethsen, K. K. & Askehave, I. (2010). PIL of the month: A study of best practice in EU patient information leaflets. Journal of Applied Linguistics & Professional Practice, 7(1), 97–120. https://doi.org/10.1558/japl.v7i1.97
Zethsen, K. K. & Montalt, V. (2022). Translating Medical Texts. In K. Malmkjær (Ed.). The Cambridge Handbook of Translation (pp. 363–378). Cambridge University Press. https://doi.org/10.1017/9781108616119.019
Data availability statement
The questionnaire used for this survey is available on the University of Vienna digital repository PHAIDRA (https://phaidra.univie.ac.at/o:2065108). The survey dataset will be made available on PHAIDRA after the completion of the author’s doctoral project.